
Quick comment on an insightful and important new Nature article on SARS-CoV-2 vaccination
The study highlights - and additionally raises - major concerns

I have been extremely busy chasing tons of new ideas and trying to get these into a publishable format :-)
However, a very recent study, published in Communications Medicine, deserves attention. Congratulations to the authors for this important work and to the journal for publishing it!
The findings are devastating, and the text is astonishingly clear!
The authors of “Association of SARS-CoV-2 vaccination status with risk of influenza-like illness and loss of workdays in healthcare workers”, based on a study of 1745 healthcare workers in Switzerland, write:
“The study found that those who recently received a COVID-19 booster were more likely to report symptoms and take sick leave. In contrast, people who received the seasonal flu vaccine were less likely to report symptoms or miss work. These findings suggest that COVID-19 boosters may not offer clear short-term benefits in a post-pandemic setting, and may even increase short-term illness risk.”
“In both analyses, we show that more SARS-CoV-2 vaccinations are associated with a higher risk of influenza-like respiratory illness and workdays lost.”
“Based on our data, we conclude that SARS-CoV-2 booster vaccination did not contribute to a measurable protection of the HCW workforce studied and may even temporarily increase the likelihood of symptomatic infection and workday loss.”
Interestingly, Fig. 2 shows that:
The percentage for at least 2 ILI episodes slightly increases with the number of doses received!
This does not necessarily mean SARS-CoV-2 infection alone. If it had been COVID-19 alone, the authors would have made this explicit. This indicates possible tolerance - possibly even an increase in tolerance - to any influenza-like respiratory illness (ILI), along with the number of shots.
I.e., it is possible that the deleterious tolerance effect may not be limited to the targeted disease!
Ironically, this is what I have been predicting as cross-tolerance: the more shots, the greater the concern for unintended tolerogenic responses towards an increasing number of non-targeted pathogens (unaccounted bystander effect): https://osf.io/preprints/osf/fjnav_v1, https://www.authorea.com/users/933419/articles/1304117-evidence-for-non-specificity-of-immune-responses-via-the-inherent-adjuvanticity-of-the-mrna-injections
What I find absolutely terrifying is that this is in a cohort (health-care workers) with ample prior exposure to respiratory pathogens! They would have had immunity.
One of my concerns (see my preprints) has been that the shots would even undermine existing natural immunity. It seems possible they may perturb prior immune learning (“imprinting”).
In this study, possibly indicative of this, the percentage for anti-N positivity goes down with the number of doses received (Table 1).
I.e., as seen from Table 1 in https://www.nature.com/articles/s43856-025-01046-8:
These health-care workers all had natural immunity to SARS-CoV-2 (97% of the unvaccinated were anti-N positive).
With an increased number of doses, natural immunity (as commonly measured in terms of anti-N Abs) goes down significantly (from 97% to 84.9% after 4 doses).
The table shows a diminished normal immune response towards other viral epitopes, here N (which are critical for natural immunity).
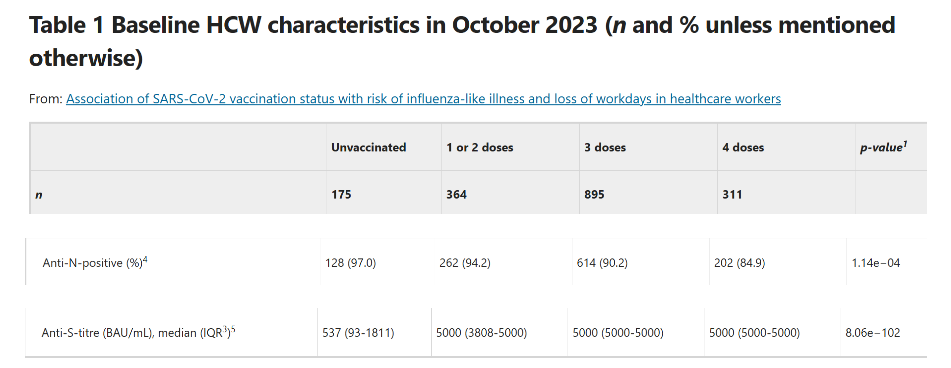
Source: https://www.nature.com/articles/s43856-025-01046-8
At the same time, as seen from the last row in the table, the anti-S antibodies following the injections run off the chart (it is possible that some of these may be IgG4 and thereby contribute to tolerance).
While I have some theories as to when/why the shots would increase (cross)-tolerance effects, the opposite is also possible. As I discuss in my preprints, this could, depending on the situation, also lead to unintended immune activation towards unintended antigens. The concern here is that of excessive immune responses and autoimmunity.
In all, you may have cross-tolerance and/or cross-priming, albeit not in a good way.
Thank you for drawing attention to this study and commenting on it. It is certainly remarkable. I am a bit confused, though, by your use of the term 'tolerance.' Immune tolerance refers to the lack of a (strong) immune response against a pathogen/antigens. That would mean that one would expect no or only mild symptoms after infection, i.e. no symptoms of ILI. Maybe it would be better to speak of a not-effective/derailed immune response. What would happen in the case of real immune tolerance? Would the virus continue to replicate and wreak havoc? On the other hand, a recent study has found that mice without B and T cells did not suffer much from SC2 infection. https://www.science.org/doi/10.1126/sciadv.adg5461. I find this quite puzzling.
"In the years following the COVID-19 pandemic, it is still unclear whether annual COVID booster vaccines are necessary for low-risk populations such as healthcare workers."... oh really, they call the authors scientists? Unfortunately, autism is related to the shots. Basics in protein-engineering are not required to understand that without a virus there is no chance for any efficacy. Even in 2025 the Swiss PDB-Viewer is not able to do a proper visualisation of Pfizer's awfully wrong designed spike-protein 6xra - like big holes in swiss cheese.